The frenulum is a small fold of mucous membrane that secures or restricts the motion of two parts; it is constituted by oral mucosa, connective and muscle fibers.
The most frequent are: medial vestibular, distinguished between upper labial and lower labial; lateral vestibular, around upper and lower premolars; medial lingual, connecting the floor of the mouth to the midline of the underside of the tongue.
Frenulum abnormalities can cause diastemata between incisors, both upper and lower incisors, and ankyloglossia due to the presence of a short, hypertrophic lingual frenulum.
The diagnosis of ankyloglossia mainly involves the impossibility to touch the roof of the mouth with the tip of the tongue, split tongue with a medial fissure on protrusion, back curvature of tongue and consequent impossibility to tongue protrusion for more than 1 or 2 cm beyond the lower incisors.
The presence of ankyloglossia also causes phonation disorders, atypical deglutition and related orthodontic problems; a flat tongue may cause excessive pressure on lower incisors and growth deficits with occlusal problems, therefore patients with ankyloglossia frequently develop over bite and class-II disorders with over jet .
|
|
|
|
|
|
|
|




Case Report
We compared the results of traditional scalpel surgery to the more frequent use of laser surgery; we noticed that, concerning lingual function and relapse, the procedures have similar results.
Their results are different concerning intraoperative complications and postoperative course; laser surgery has the advantage of a clean operative field after surface incision, without bleeding and sutures.
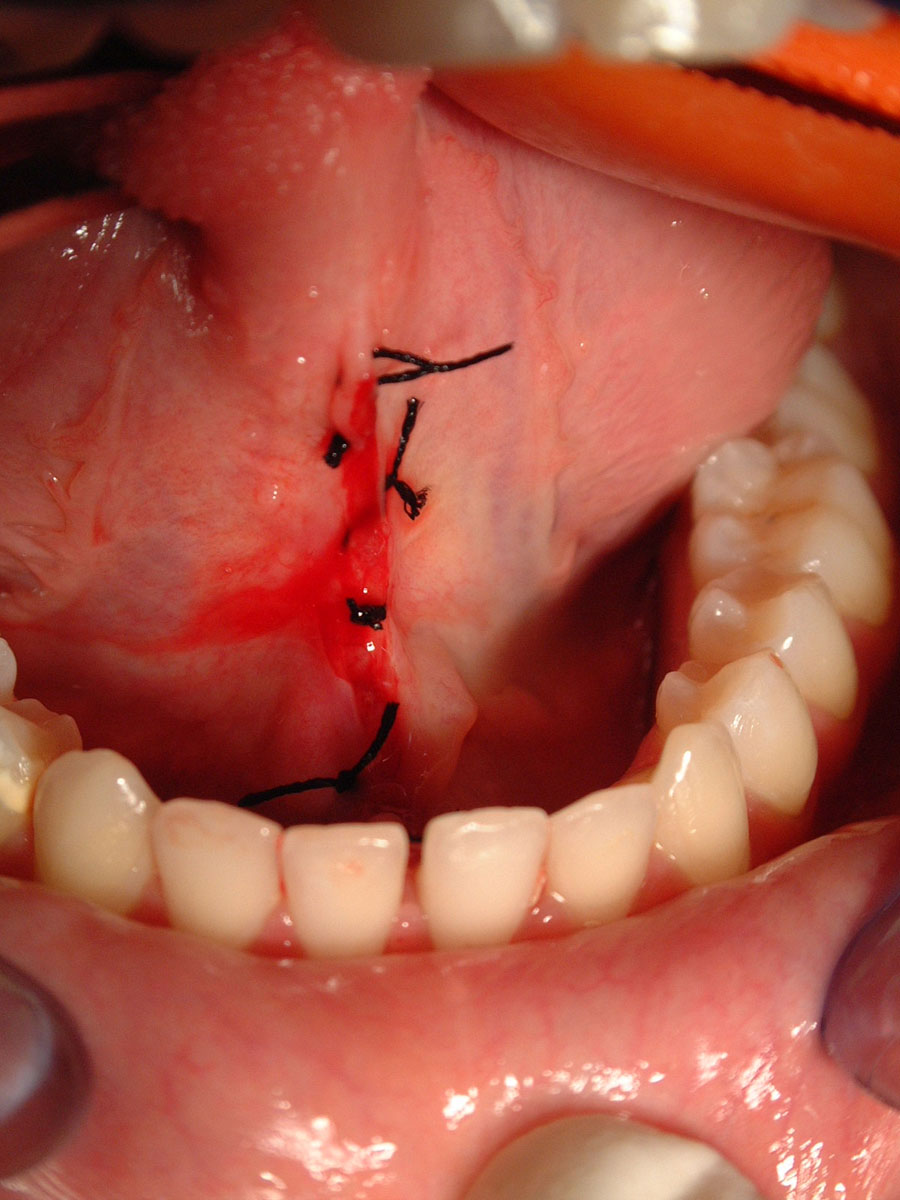
The first clinical case is a 14-year-old female patient with short lingual frenulum and phonation disorders. After a few drops of anesthetic to the side of the frenulum, we performed 5-point v-shaped sutures and sectioned the soft tissues of frenulum with a scalpel.
Tissue lateral to the margin of the wound was undermined by sharp and blunt dissection, and then sutured without tension. After removal of lingual frenulum, the tongue can soon extend up and out of the mouth, without split tongue and back curvature. Finally, we performed an interrupted suture.
The second clinical case is a 13-year-old female patient with atypical deglutition and short frenulum, who received frenulectomy and rehabilitation therapy of lingual movements; we then used lidocaine spray as anesthetic and performed laser root incision in the frenulum central area.
To avoid relapse, we made a small lateral incision, approximately 1 cm for each side; then we disinfected the area with chlorhexidine topical gel and used aminogam gel to favour reepithelization.
Congresso Nazionale dei Docenti di Discipline Odontostomatologiche e Chirurgia Maxillo Facciale
Firenze – Siena, 14-16 Aprile 2011
Università degli Studi di Bari Dipartimento di Odontostomatologia e Chirurgia
Direttore: Prof.ssa D. DE VITO
Calabrodental S.r.l. Unità Operativa di Chirurgia Maxillo-Facciale Regione Calabria – Crotone Dir. San: Dott. M. W. Marrelli
AUTHORS
INCHINGOLO F.; INCHINGOLO A.D.; DIPALMA G.; PALLADINO A.; TATULLO M.; INCHINGOLO A.M.; MARRELLI M.
BIBLIOGRAFY
2. Chu MW, Bloom DC.; [Posterior ankyloglossia: a case report] Int J Pediatr Otorhinolaryngol. 2009 Jun;73(6):881-3. Epub 2009 Mar 20.
3. Marenzi G, Urciuolo V, Cimmino P, Cirillo A, Sammartino G.; [Frenulectomy: proposal of a new surgical approach and case report]Minerva Stomatol. 2011 Jan-Feb;60(1-2):51-6.
4. De Benedittis M., Petruzzi M., Pastore L., Inchingolo F., Serpico R.; [Nd: YAG laser for gingivectomy in Sturge-Webber syndrome] J Oral Maxillofac Surg. 2007 Feb; 65(2):314-6