Odontochondrodysplasia (OCDC) is a chondrodysplasic disease. More specifically, it is a genetically transmitted, generalized spondylometaphyseal dysplasia (SMD). Among the clinical evidences associated to this syndrome, we can find all the clinical signs of SMD 1 : pectus carinatum, joint hyperextensibility, coxa valga and genu valgum, upper and lower limb asymmetry, and vertebral abnormalities. The association between dentinogenesis imperfecta and a definite form of SMD was first reported by Goldblatt 2, which is the reason why this particular form of dysplasia is also called Goldblatt syndrome.
CASE REPORT
The patient was a 19-year-old Caucasian female, who had a normal birth and outbred healthy parents with no significant disease. Her father had a height of 173 cm, and her mother had a height of 167 cm. The patient’s case history revealed that from birth, she has been under medical supervision for lower-limb dysmetria (left lower limb 15 cm longer than the right lower limb), associated with short stature, mandibular hypoplasia, and bilateral epicanthus.
However, specialist reports confirmed a delayed growth of bone segments. Clinical and radiographic examinations revealed a narrow, prominent chest, signs of rachitis with facies sui generis, shortness of long bones, metaphyseal irregularity in the proximal femur, shortness of the neck of the femur, thoracic scoliosis convex to the right with square vertebral bodies. The patient came to our attention at the age of 17, with a weight of 40 kg and a height of 140 cm.
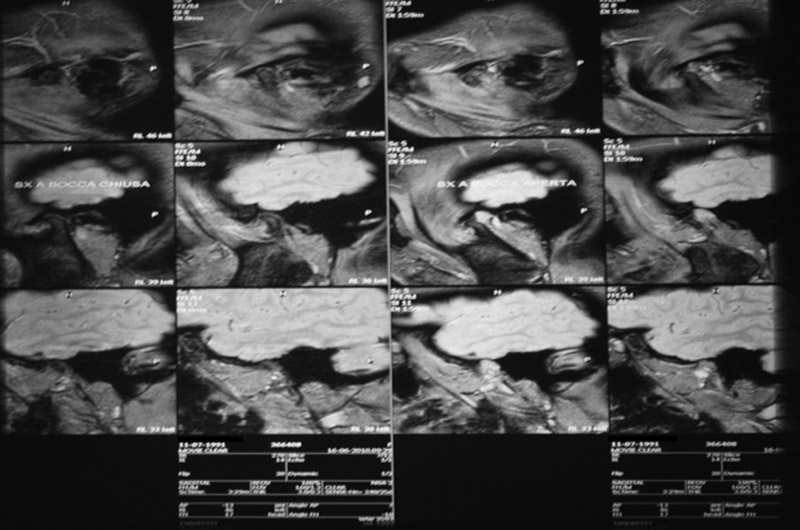
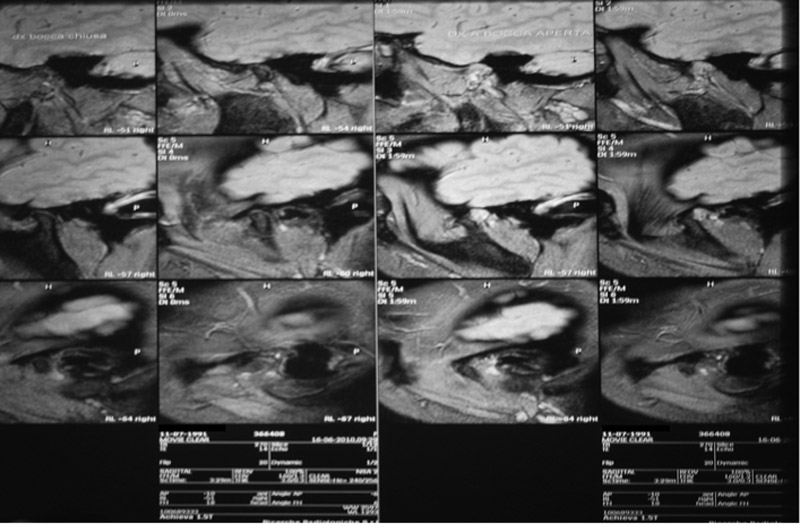
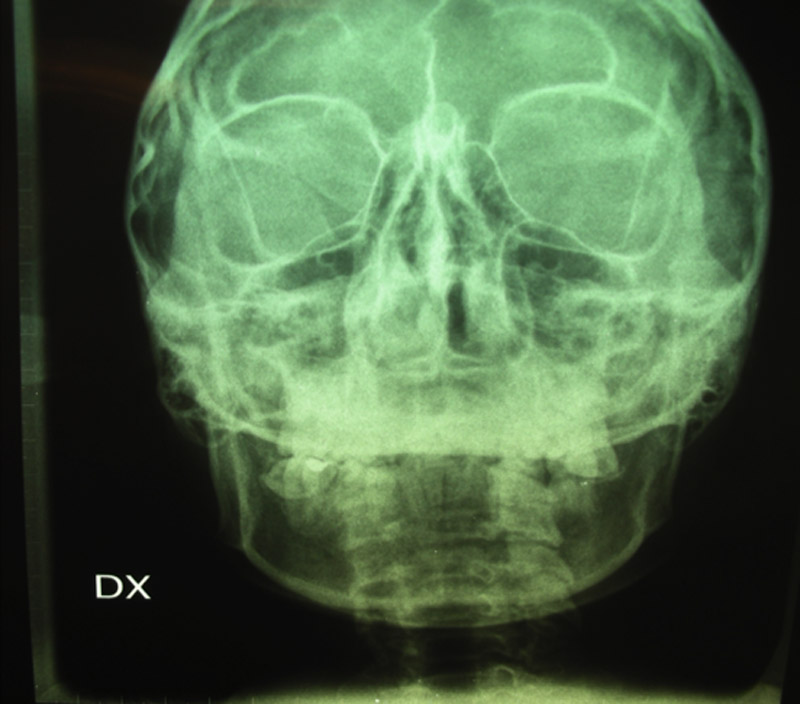
To carry out a careful analysis of the clinical picture, we conducted several clinical investigations. First of all, radiographic examinations such as chest x-ray, hand x-ray, spine x-ray in 2 projections, lower limb x-ray with pelvis in 1 projection, NMR of the temporomandibular joint (TMJ) without contrast medium (fig.1), telecranium x-rays in posteroanterior projection (fig.2), orthopantomography (OPT) of dental arches (fig.3) and telecranium x-rays in laterolateral. Besides, alginate dental impressions were taken and then poured into gypsum molds.
|
|
|
|
| Figure 1 Open-mouth and closed-mouth NMR (right and left) in TMJ dynamic study |
Figure 2 Posteroanterior projection x-ray |
|
CEPHALOMETRIC STUDY
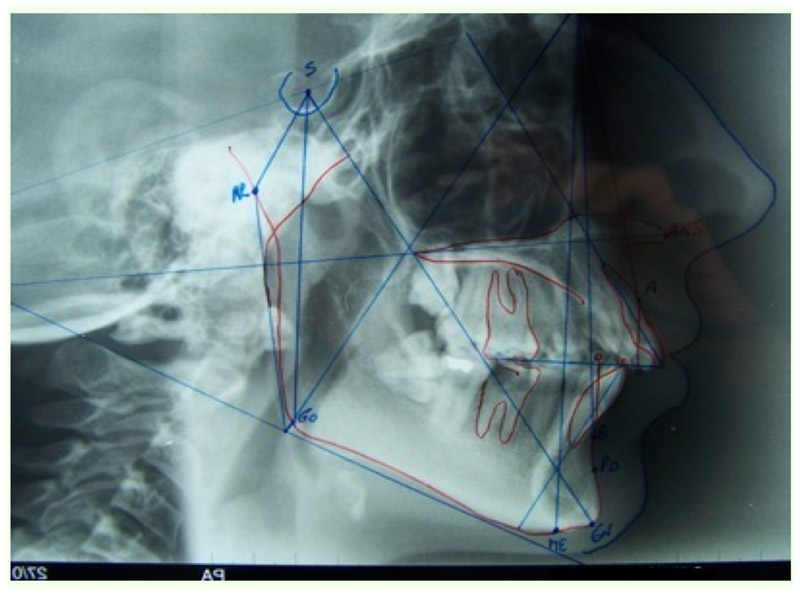
Laterolateral and posteroanterior telecranium x-rays (fig.4), supported by gypsum molds, allowed us to obtain cephalometric data according to Jarabak’s cephalometric analysis 3, which outlined a clinical picture of Goldblatt Syndrome.
The orthodontic diagnosis clearly defines a II class/II division (Angle’s classification) in a hyperdivergent patient 4. In our patient with OCDC, hyperdivergence was measured through the cephalometric values.
The sum of angles at the cranial base, which is the sum of angles NSAr/SArGo/ArGoMe, was 409º; the percentage height of the facial skeleton, which is posterior facial height multiplied by 100, divided by anterior facial height, was 61.1%; the lower gonial angle was 87º; the position of the mandible compared to the cranial base (NSGn, y-axis), was 79º; the intermaxillary angle, existing between maxilla (MX) and mandible (MB) and expressed as MX/MB rate, was 30º.
|
|
 |
| Figure 3 Orthopantomography (OPT) |
Figure 4 Cephalometric tracing performed on a latero-lateral projection teleradiography of the skull. |
 |
|
| Figure 5 Patient’s face |
Figure 6 Patient’s occlusion |


Another fundamental element of the cephalometric analysis was the patient’s skeletal class II, showed by the difference SNA-SNB = ANB, which was 8º, as confirmed by Witz index (A0/B0) indicating the intermaxillary rate, which was 9 mm (values higher than 4 mm indicate a basal class II). Besides, the angle A-Na-Pog, indicating the protrusion of the upper jaw with relation to total profile, was 8º.
The angle Ans-Na-Pog, showing the position of the body of maxilla with relation to the body of mandible, was 18º. These results indicate an evident skeletal class II. Linear measurements of the skeletal structures were performed, which showed that the length of the anterior cranial base was 16 mm shorter than n.v., the length of the body of mandible was 10 mm lower than n.v., and the length of the lateral cranial base was 5 mm shorter than n.v. 5.
Congresso Nazionale dei Docenti di Discipline Odontostomatologiche e Chirurgia Maxillo Facciale
Firenze – Siena, 14-16 Aprile 2011
Università degli Studi di Bari Dipartimento di Odontostomatologia e Chirurgia
Direttore: Prof.ssa D. DE VITO
Calabrodental S.r.l. Unità Operativa di Chirurgia Maxillo-Facciale Regione Calabria – Crotone Dir. San: Dott. M. W. Marrelli
AUTHORS
PALLADINO A. * ; INCHINGOLO F. ; DE CAROLIS M. ; DIPALMA G. ; INCHINGOLO A. M. ; INCHINGOLO A. D. ; TATULLO M.
BIBLIOGRAFY
1. P Beighton. Spondyloepimetaphyseal dysplasia with joint-laxity (SEMDJL). I Med Genet, 1994; 31:136-140.
2. J. Goldblatt, P. Carman, P. Sprague. Unique dwarfing, spondylometaphyseal skeletal dysplasia, with joint
laxity and dentinogenesis imperfecta. Am J Med Genet, May 1 1991; 39(2):170-2.
3. Jarabak, J.R.: Technique and Treatment with the Light Wire Appliance. C.V. Mosby Co. St. Louis, 1963.
4. William R. PROFFIT “Ortodonzia moderna” Second edition, Masson, 2001.
5. Tweed C.F.: "Clinical Orthodontics." C.V. Mosby, St Louis, 1966.